Detection of Mycobacterium Tuberculosis IgM and IgG Antibodies and Associated Risk Factors Among Apparently Healthy Undergraduate Students of a Private University in South-West Nigeria
Abstract
Background: Infection with Mycobacterium tuberculosis (TB) is frequent among Nigerians. Many people are infected without realizing it (asymptomatic) and thus provide a risk of transmission to others. Not only will early treatment prevent TB complications, but it will also help to break the infection cycle in a community.
Objective: The study was conducted to determine the prevalence of Mycobacterium tuberculosis IgM and IgG antibodies and associated risk factors among apparently healthy undergraduate Students of Babcock University, Ilishan-Remo, Ogun State.
Methodology: The serum samples of 100 consenting participants were collected randomly and screened for TB antibodies using Aria TB IgG/IgM Combo Rapid Antibody Test Cassette (CTK Biotech Inc. Poway, CA 92064, USA). A structured questionnaire was administered to consenting students to obtain information on their bio-data (e.g, the age, sex, study level etc.), as well as clinical information regarding their health (History of TB, history of BCG vaccination, use of anti-TB medications, alcohol consumption, smoking habits etc.).
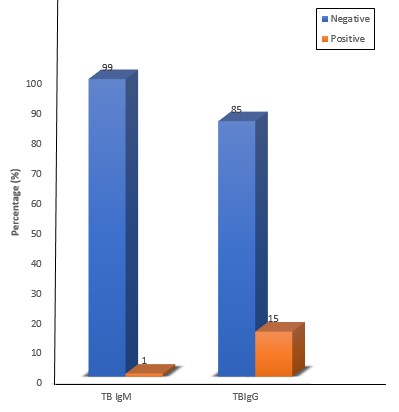
Results: The outcome of this study shows that 15 (15%) out of the 100 participants screened, were positive for TB IgG antibody, while, only 1 (1%) person was positive for TB IgM antibody. There was no significant association (P>0.05) between percentage TB IgG positivity and the socio-demographic characteristics of the study participants (gender, age, study level and tribe), except for religion. The percentage of TB IgG positivity among the study participants was found to be significantly higher than of TB IgM positivity (P<0.05). None of the 15 participants who tested positive to TB IgG indicated any of the signs and symptoms (persistent cough, chest pain, nausea, fever, chills, loss of appetite, fatigue and night sweat) associated with TB), however the only person who tested positive for TB IgM indicated all, except night sweat. Identified risk factors associated with the occurrence of TB IgM include history of TB, lack of BCG vaccination, history of diabetes and physical unfitness.
Conclusion: The findings of this study show that asymptomatic and latent tuberculosis infection exists among the study participants, and that if left untreated, it will progress to active tuberculosis with all of its associated complications, including death. This emphasizes the importance of ongoing public health education, BCG vaccination, and periodic screening to detect asymptomatic cases in the study population in order to break the infection cycle.
References
[2] Solomon, B. A., Hannah, B., & Etefia, E. (2019). The Occurrence of Mycobacterium tuberculosis Among Students Living at The University of Calabar Hostels, Calabar, Nigeria. Mintage Journal of Pharmaceutical and Medical Sciences, 8(4), 14-15.
[3] Cruz, A., & Starke, J. (2014). Tuberculosis. In Cherry J, HarrisonG, Kaplan S, Steinbach W, Hotez P (ed), Feigin and Cherry’s textbook of pediatric infectious diseases. Elsevier Saunders, Philadelphia, PA. p 1335-1380.
[4] World Health Organization (WHO). (2010). Global Tuberculosis Control. Retrieved January 18th 2021, from https://apps.who.int/iris/handle/10665/44425
[5] World Health Organization (WHO). (2009). “Epidemiology”. Global Tuberculosis Control and Strategy. “WHO/HTM/TB/2009.426”. Assessed on the 18th of January, 2021.
[6] World Health Organization (WHO). (2017): Global Tuberculosis Report, www.who.int. Assessed on the 18th of January, 2021.
[7] Dunn, J. J., Starke, J. R., & Revell, P. A. (2016). Laboratory Diagnosis of Mycobacterium tuberculosis Infection and Disease in Children. J. Clinical Microbiolgy, 54, 1434-1441.
[8] Narasimhan, P., Wood, J., MacIntyre, C. R., & Mathai, D. (2013). Risk Factors for Tuberculosis, Pulmonary Medicine, 9, 828-939.
[9] Amicocante, M. (2010). Rational use of immunodiagnostic tool for tuberculosis infection: guidelines and cost-effective studies. Journal of the Italian Society for Medical Virology, 33(2), 93-107.
[10] Marie, A. P., & Niemeier, T. R. (2014). Evaluation of Exposure Tuberculosis among Employees at Medical Center. J. occup. Environ. Hyg., 11(6), 63-68.
[11] Chinedu, A.N., Seema, B., & Gladys, A. O. (2008). Prevalence of Mycobacterium tuberculosis antibodies in a healthy population in a South-Eastern State of Nigeria. J. Pak Med Assoc., 58(1), 8-10.
[12] World Health Organization (WHO). (2006). Global Tuberculosis control: country profile-Nigeria. pp 107-109. Assessed on the 5th of April, 2021.
[13] Devi K. R. U., Ramalingam, B., Brennan, P. J., Narayanan, P. R., & Raja, A. (2001). Specific and early detection of IgG, IgA and IgM antibodies to Mycobacterium tuberculosis 38kDa antigen in pulmonary tuberculosis. Tuberculosis, 81(3): 249-253.
[14] Bam, N., & Karn, R. (2009). IgM and IgG Antibodies in Tuberculosis, Journal of Institute of Medicine, 31(3): 34-36.
[15] Wang, S., Wu, J., Chena, J., Gaoa, Y., Zhanga, S., Zhoub, Z., Huangb, H., Shaoa, L., Jina, J., Zhanga, Y., & Zhanga, W (2018). Evaluation of Mycobacterium tuberculosis-specific antibody responses for the discrimination of active and latent tuberculosis infection. International Journal of Infectious Diseases, 70 (18): 1-9.
[16] Feng, X., Yang, X., Xiu, B., Qie, S., Dai, Z., Chen, K., Zhao, P., Zhang, L., … Zhang, H. (2014). IgG, IgM and IgA antibodies against the novel polyprotein in active tuberculosis. BMC Infectious Diseases, 14(336), 2-9.
[17] Narasimhan, P., Wood, J., MacIntyre, C. R., & Mathai, D. (2013). Risk Factors for Tuberculosis, Pulmonary Medicine, 9, 828-939.
[18] AL-Khafaji, J. K. T. (2014). Characterization of Mycobacterium tuberculosis and Predisposing Factors Associated with Tuberculosis Among Risk Population in Baghdad City, Journal of Babylon University/Pure and Applied Sciences, 9(22), 2548.
[19] Chan, E. D., Reves, R., Belisle, J. T., Brennan, P. J., & Hahn, W. E. (2000). Diagnosis of Tuberculosis by a Visually Detectable Immunoassay for Lipoarabinomannan. American Journal of Respiratory and Critical Care Medicine, 161, 1713-1719.
[20] Arce-Mendoza, A. Y., Rosas-Taraco, A. G., Cantú Treviño, M. P., Limón-Flores, A. Y., … Rafael, González-Álvarez (2018). Efficacy of ELISA test in diagnosis of Mycobacterium tuberculosis infection. Microbiology Research International, 6(10), 20-27.

This work is licensed under a Creative Commons Attribution 4.0 International License.
Copyright for this article is retained by the author(s), with first publication rights granted to the journal.
This is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).








1.png)